

The Weight Loss Shot That Outperforms Gastric Bypass Surgery
I have been practicing obesity medicine for over a decade and have watched this field transform more in the last five years than in the previous twenty. So I say without hesitation that the Phase 3 trial results for retatrutide, Eli Lilly's next-generation injectable, are the most remarkable data I have seen come out of this space. It’s producing weight loss numbers that have historically belonged only to bariatric surgery! So let’s dive in on what you need to know.
What Is Retatrutide?
Retatrutide is a once-weekly injectable developed by Eli Lilly that works on three hormone receptor pathways simultaneously: GLP-1, GIP, and glucagon. Every currently approved weight loss medication works on one or two of these pathways. The dual GLP-1/GIP mechanism of tirzepatide (Zepbound) was a major step forward. But adding glucagon receptor activation introduces a third lever that increases energy expenditure and drives additional fat loss beyond what dual agonists can achieve. That triple mechanism is why the efficacy numbers look the way they do.
What the Phase 3 Data Show
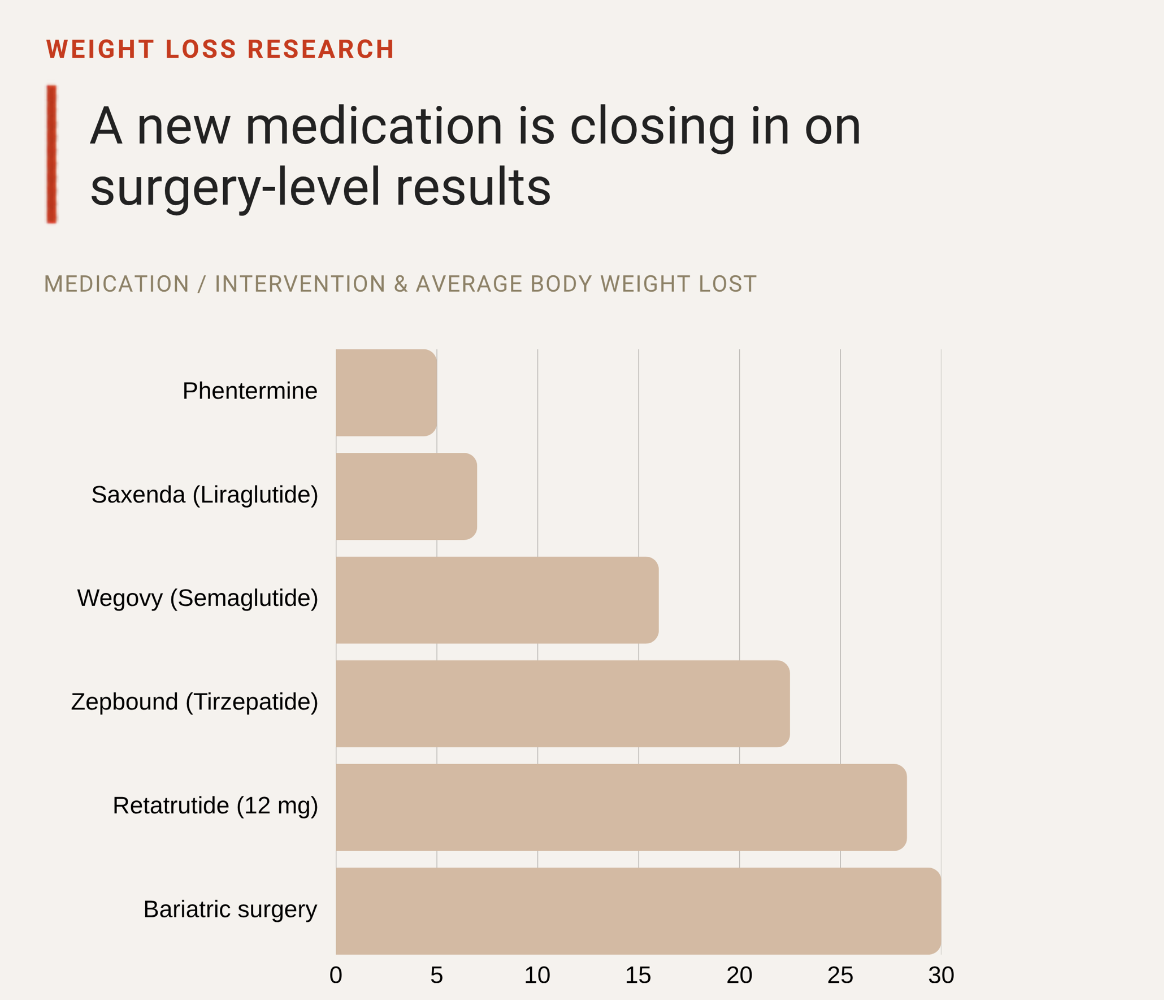
Results from the TRIUMPH-1 Phase 3 trial, released in May 2026, showed patients on the highest 12 mg dose lost an average of 70.3 pounds, representing 28.3% of their starting body weight over 80 weeks. Nearly half of participants at that dose achieved 30% or more weight loss.
The 4 mg dose, which requires only a single escalation step and may be better tolerated, still produced an average of 47.2 pounds of weight loss, or 19% of body weight.
For context: the best currently approved medication, Zepbound, produces average weight loss of approximately 22.5% of body weight. Retatrutide's highest dose clears that bar by a significant margin. Lilly's own chief scientific officer described 30% weight loss as a number previously only associated with bariatric surgery.
Beyond the scale, retatrutide also reduced liver fat by up to 50% in study participants, which is why Lilly added a dedicated NASH trial to the Phase 3 program. Blood pressure, triglycerides, fasting glucose, and A1C all improved across dose groups as well.
Tolerability and Side Effects
The side effect profile aligns with the GLP-1 class. Nausea, diarrhea, vomiting, and constipation were the most commonly reported adverse events. Importantly, the majority of participants completed the trial, which signals that side effects were manageable for most patients when dose escalation was handled carefully.
As with all agents in this class, slow titration is important. Patients who escalate too quickly experience significantly more gastrointestinal burden. The 4 mg dose option, with its simpler escalation pathway, may offer a better-tolerated entry point for patients who are sensitive to GI side effects. The standard class-level counseling applies: monitor for signs of thyroid concerns, pancreatitis symptoms, and changes in heart rate.
Where Retatrutide Stands Out
No approved medication has produced average weight loss of 28% in a controlled trial. The closest comparison is Zepbound at approximately 22.5%. The gap between those two numbers is clinically meaningful, particularly for patients with severe obesity who need substantial weight reduction to improve comorbidities like type 2 diabetes, hypertension, sleep apnea, and joint disease. Lilly is running a direct head-to-head comparison between retatrutide and tirzepatide, with results expected in late 2026 or early 2027. That data will help clarify which patients benefit most from which agent.
Injectable GLP-1 and Incretin-Based Medications
Zepbound (tirzepatide, weekly injection) is currently the most effective approved option at approximately 22.5% average weight loss. Targets GLP-1 and GIP receptors. Also marketed as Mounjaro for type 2 diabetes management.
Wegovy HD (semaglutide 7.2 mg, weekly injection) was approved in March 2026. Average weight loss approximately 20.7% of body weight, making it a stronger option than the original Wegovy formulation for patients who need more aggressive intervention.
Wegovy (semaglutide 2.4 mg, weekly injection) approved in 2021, average weight loss approximately 15% to 17% of body weight over 68 weeks. Approved for adults and adolescents aged 12 and older with obesity.
Saxenda (liraglutide, daily injection) approved in 2014, average weight loss approximately 5% to 8%. A once-daily injection that is less commonly initiated now given the availability of more effective weekly options, but still appropriate for certain patients.
Oral GLP-1 Medications
Foundayo (orforglipron, daily tablet) approved April 2026. The only oral GLP-1 that can be taken any time of day without food or water restrictions. Average weight loss approximately 11% of body weight at the highest dose. Also demonstrated improvements in blood pressure, cholesterol, and triglycerides.
Oral Wegovy (semaglutide 25 mg tablet, daily) approved December 2025. Average weight loss approximately 16.6% of body weight. Requires fasting and specific fluid conditions at time of dosing.
Older Oral Medications
Qsymia (phentermine/topiramate extended-release) approved 2012. Combines a stimulant appetite suppressant with a centrally acting medication. Average weight loss approximately 7% to 9% of body weight.
Contrave (naltrexone/bupropion) acts centrally to reduce appetite and cravings. Average weight loss approximately 5% of body weight. A reasonable option for patients with comorbid depression or alcohol use history. Contraindicated with opioid use and seizure disorders.
Xenical / Alli (orlistat) blocks dietary fat absorption in the gastrointestinal tract. Average weight loss approximately 3% to 5% above placebo. Available as prescription Xenical or over-the-counter Alli. Gastrointestinal side effects with fat-containing meals limit adherence for many patients, but it remains a low-cost option where appropriate.
Phentermine is approved for short-term use only, typically up to 12 weeks. Inexpensive and produces meaningful short-term appetite suppression. Not appropriate for long-term chronic disease management. Contraindicated in patients with cardiovascular disease.
What This Means for Clinical Practice
Retatrutide represents the most significant advance in obesity pharmacotherapy since tirzepatide. Producing surgical-level weight loss in a once-weekly injectable would fundamentally shift how we think about the treatment algorithm for patients with severe obesity. For patients who need the most aggressive pharmacological approach currently on the market, Zepbound remains the standard. For patients who prefer or require an oral option, Foundayo and oral Wegovy are good options.